Mary Madison, RN, RAC-CT, CDP
Clinical Consultant – Briggs Healthcare
The GAO (Government Accountability Office) released this report on Monday, February 5, 2018. “GAO was asked to examine state and federal oversight of assisted living services in Medicaid. This report (1) describes state spending on and coverage of these services, (2) describes how state Medicaid agencies oversee the health and welfare of beneficiaries in these settings, and (3) examines the extent that CMS oversees state Medicaid agency monitoring of assisted living services.”
GAO-18-179 is a 52-page report that should be reviewed by all Assisted Living owners and management teams. The findings of the GAO call for improved state reporting of critical incidents and more guidance/enforcement needed from CMS on the information that states must report.

Above are just 4 of the charts/graphs in this data-rich report
GAO offers these conclusions:
- CMS’s ability to effectively monitor how well states are assuring beneficiary health and welfare is limited by gaps in state reporting to CMS.
- CMS has not provided clear guidance to states on what information to include in annual reports on deficiencies they identify. As a result, CMS lacks assurance that it is receiving consistent, complete, and relevant information on deficiencies that is needed to oversee beneficiary health and welfare. Lacking clear guidance on the reporting of deficiencies may result in a delayed recognition of problems that may affect beneficiary health and welfare.
- CMS has not ensured that all states submit annual reports on their HCBS waiver programs as required. Without improvements to state reporting, CMS cannot ensure states are meeting their commitments to protect the health and welfare of Medicaid beneficiaries receiving assisted living services, potentially jeopardizing their care.
GAO provides three recommendations to CMS:
- The Administrator of CMS should provide guidance and clarify requirements regarding the onitoring and reporting of deficiencies that states using HCBS waivers are required to report on their annual reports.
- The Administrator of CMS should establish standard Medicaid reporting requirements for all states to annually report key information on critical incidents, considering, at a minimum, the type of critical incidents involving Medicaid beneficiaries, and the type of residential facilities, including assisted living facilities, where critical incidents occurred.
- The Administrator of CMS should ensure that all states submit annual reports for HCBS waivers on time as required.
Why is this report important?
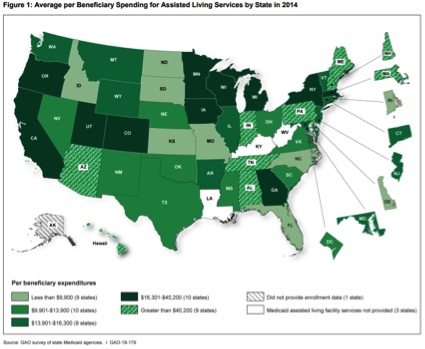
“State Medicaid agencies in 48 states that covered assisted living services reported spending more than $10 billion (federal and state) on assisted living services in 2014. These 48 states reported covering these services for more than 330,000 beneficiaries through more than 130 different programs. Most programs were operated under Medicaid waivers that allow states to target certain populations, limit enrollment, or restrict services to certain geographic areas…HCBS expenditures grew from $81 billion in FY 2014 to $87 billion in FY 2015 (a seven percent increase), accounting for all the growth in expenditures in FY 2015 for long-term services…State Medicaid agencies are required to protect beneficiary health and welfare and operate systems to monitor for critical incidents—cases of potential or actual harm to beneficiaries such as abuse, neglect, or exploitation.
- Twenty-six state Medicaid agencies could not report to GAO the number of critical incidents that occurred in assisted living facilities, citing reasons including the inability to track incidents by provider type (9 states), lack of a system to collect critical incidents (9 states), and lack of a system that could identify Medicaid beneficiaries (5 states).
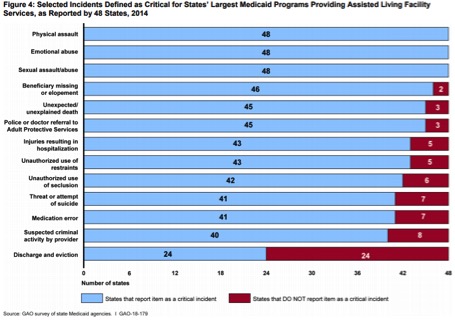
- State Medicaid agencies varied in what types of critical incidents they monitored. All states identified physical, emotional, or sexual abuse as a critical incident. A number of states did not identify other incidents that may indicate potential harm or neglect such as medication errors (7 states) and unexplained death (3 states).
- State Medicaid agencies varied in whether they made information on critical incidents and other key information available to the public. Thirty-four states made critical incident information available to the public by phone, website, or in person, while another 14 states did not have such information available at all.”
Additional information can be found at this link.

One thought on “Improved Federal Oversight of Beneficiary Health and Welfare Is Needed in Medicaid ALFs”
Comments are closed.