Mary Madison, RN, RAC-CT, CDP
Clinical Consultant – Briggs Healthcare

January 3, 2023 … MACPAC (Medicaid and CHIP Payment and Access Commission), a non-partisan legislative branch agency that provides policy and data analysis and makes recommendations to Congress on Medicaid programs, released this 19-page report that is worth your attention. I encourage you to share it with your team and colleagues.
“Medicaid is the primary payer for most nursing facility residents, but information about Medicaid payment rates is limited. The net payments a nursing facility receives consist of base payments, which are typically paid on a per diem basis, and supplemental payments, which are generally paid in a lump sum, reduced by provider contributions to the non-federal share of their Medicaid payments.
In this brief, we present estimates of 2019 Medicaid base payments across states compared to facility costs, using a standard methodology developed based on feedback from a technical expert panel convened by MACPAC in 2022. Overall, we find that:
• Across states, average base Medicaid payment rates for nursing facility services varied considerably, ranging from 62 to 182 percent of the national average, after adjusting for differences in area wages and resident acuity. This variation is similar to what has been observed with Medicaid physician and hospital base payments (MACPAC 2017; Zuckerman et al. 2017).
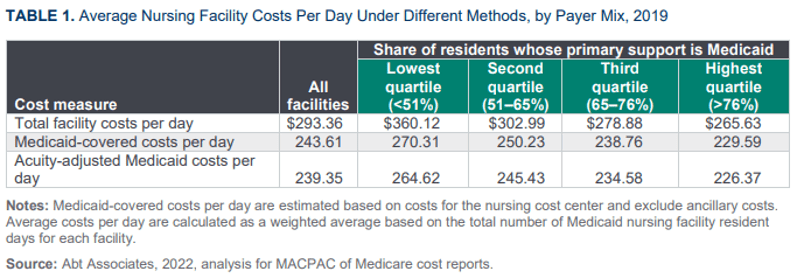
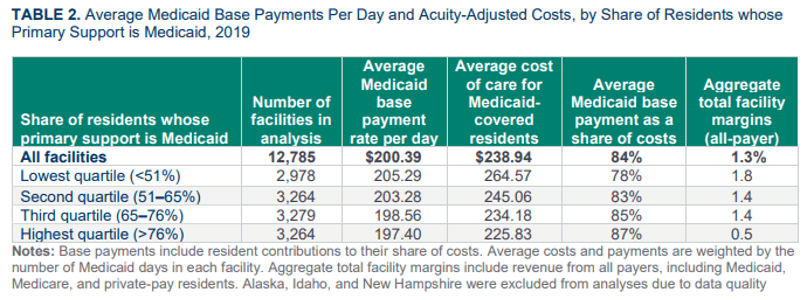
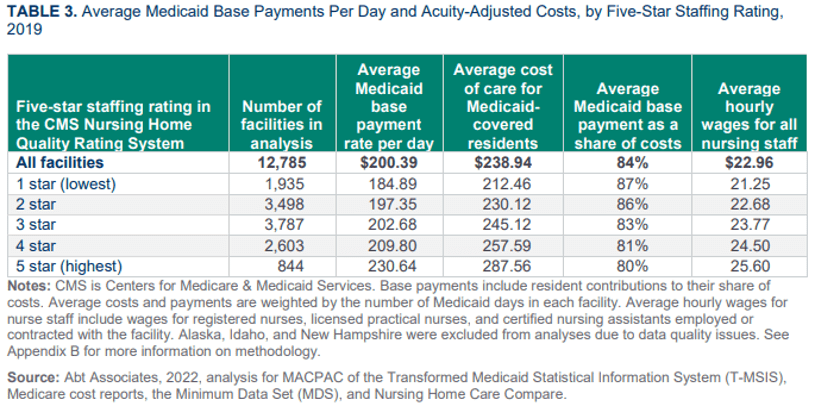
• Across facilities within states, base payment rates and costs also vary considerably. Facilities that serve a high share of Medicaid-covered residents generally have lower base payment rates but also have lower facility costs, in part because they generally have lower staffing levels than other facilities.
• Measures of base payments relative to costs vary widely, ranging from less than 70 percent of costs for 15 percent of facilities to more than 100 percent of costs for 19 percent of facilities. The median Medicaid base payment rate in 2019 was 86 percent of reported facility costs.
In addition to considering base payment rates (the amount that nursing facilities are paid per day for a specific resident), it is also important to consider supplemental payments, which are lump sum payments that some facilities receive in addition to base payments. In 2019, supplemental payments to nursing facilities totaled $3.4 billion (MACPAC 2020a). In states with available data, we find that supplemental payments can substantially affect measures of Medicaid nursing facility payments relative to costs, but unfortunately, complete data on supplemental payments to nursing facilities are not yet available at the facility level. In addition, we lack facility level data on the amount of funding that nursing facilities contribute toward the non-federal share of their Medicaid payments, which reduces the net payments that providers receive.
The issue brief begins by reviewing background information on Medicaid coverage and payment for nursing facility services and the challenges of accurately measuring the costs of care for Medicaid-covered residents. It concludes by summarizing our estimates of Medicaid base payments relative to costs and discussing the limits of available data. Additional state-specific results are included in Appendix A, and more information about the methods for this analysis are described in Appendix B.”
“This analysis shows that Medicaid nursing facility payments vary widely both across states and across facilities within a state. Although Medicaid payment rates are generally lower than other payers, Medicaid payments appear to exceed the costs of care for Medicaid-covered residents in some facilities.
This analysis also demonstrates the challenges in using costs as a benchmark for assessing Medicaid payment adequacy. We found that facilities with lower staffing rates generally have lower costs, which affects measures of Medicaid payments relative to costs for these facilities. We were not able to examine the effects of related-party transactions and other practices that may artificially inflate the costs reported on Medicare cost reports. States have the flexibility to develop their own Medicaid cost reports that could potentially be used to examine these issues in more detail, but because state definitions of allowable costs differ, it is difficult to use state cost reports to compare payment rates and costs across states.
Finally, this analysis reinforces MACPAC’s longstanding concern about the need for additional payment and financing data at the facility level, especially for supplemental payments. Such data are needed to provide a complete understanding of all types of Medicaid payments to nursing facilities, which can help inform assessments of the link between payment and access, quality, and value.”
Also worth your attention is the joint statement from these nursing home resident advocacy organizations:

